
TL;DR:
- Therapist burnout, characterized by emotional exhaustion and depersonalization, can harm treatment quality and client progress. It is often caused by high caseloads, administrative overload, and systemic issues, especially in California’s demanding mental health landscape. Clients and agencies can help prevent burnout by asking about supervision, pacing, and organizational support to ensure lasting, effective care.
Therapy is supposed to be a safe place to heal. But there’s a hidden factor that can quietly chip away at your progress before you even realize it: burnout. 89% of California mental health professionals report moderate to severe burnout, and that number should matter deeply to anyone seeking help for anxiety, depression, or trauma recovery. When a therapist is running on empty, the quality of care shifts in ways that clients often mistake for their own lack of progress. This article breaks down what burnout in therapy actually looks like, why it’s so widespread in California, and what you can do to protect your healing journey.
Table of Contents
- Defining burnout in therapy: What it means for you
- What causes burnout in therapy? Underlying factors and stressors
- Burnout in therapy: Not just a ‘therapist problem’
- Prevention and action: What you can do to protect the therapy process
- Debates and challenges: Is burnout just an individual problem?
- Why addressing burnout in therapy means changing the whole system
- Get support from burnout-aware therapy providers in California
- Frequently asked questions
Key Takeaways
| Point | Details |
|---|---|
| Burnout impacts therapy results | Therapist burnout can lead to lower-quality outcomes and early dropout for clients seeking help in California. |
| Know the warning signs | Look for emotional exhaustion or detachment in therapy sessions as signs of possible burnout. |
| Prevention includes teamwork | Clients and therapists working together with practical strategies help minimize burnout’s effects. |
| Systemic change needed | Lasting improvement requires addressing both individual self-care and changes in therapy workplace conditions. |
Defining burnout in therapy: What it means for you
Most people think of burnout as a workplace problem for overworked employees. In the therapy world, the stakes are much higher. Understanding what burnout truly means in a clinical setting helps you recognize when something isn’t working, and why.
Therapist burnout is a psychological syndrome with three core dimensions: emotional exhaustion, depersonalization, and reduced personal accomplishment. Emotional exhaustion is the depletion of inner resources after absorbing intense emotional content from clients day after day. Depersonalization means the therapist begins to emotionally distance themselves, sometimes becoming cynical or detached toward the very people they’re trying to help. Reduced personal accomplishment shows up as a loss of confidence and meaning in the work.
“Burnout is not a badge of honor, nor a private struggle. It’s a signal that the system supporting care has broken down, and clients are rarely shielded from the fallout.”
In real-world therapy, these dimensions don’t announce themselves clearly. A therapist experiencing emotional exhaustion might still show up and conduct sessions, but their responses feel less present, their attention more scattered. Understanding the therapy session structure and what engaged care actually looks like helps you notice these subtle shifts.
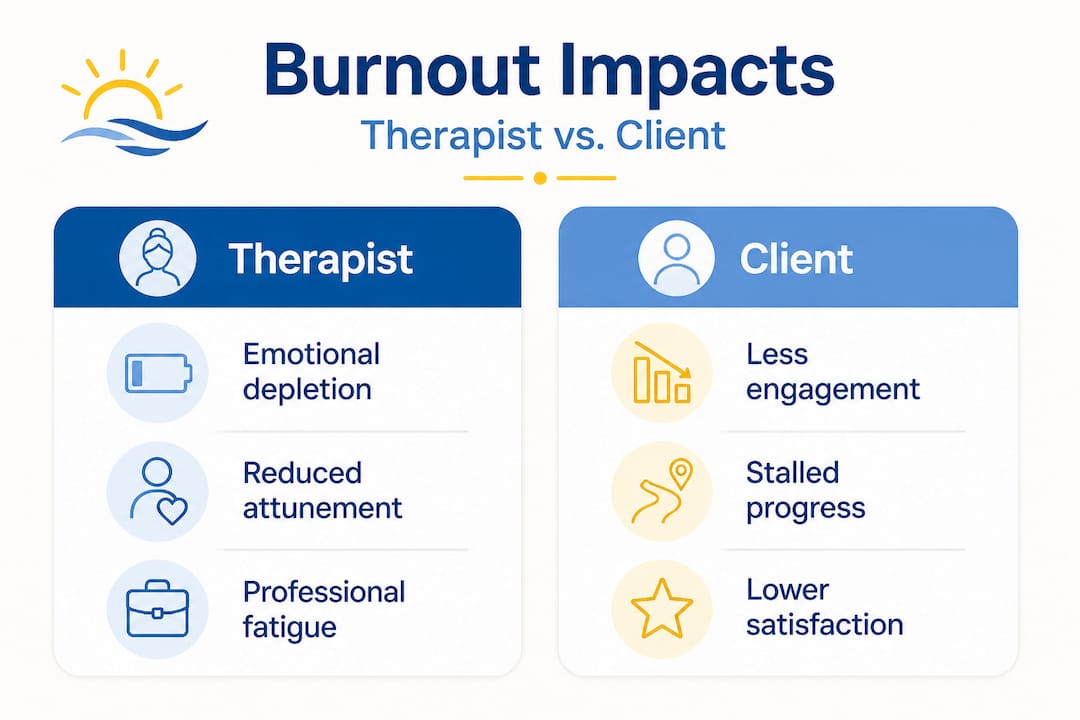
How burnout plays out for clients:
- Sessions feel formulaic or going through the motions
- Feedback from your therapist seems generic or disconnected from your specific situation
- You leave sessions feeling unheard or confused about the direction of your care
- Progress stalls after a period of early gains
- You notice your therapist seems distracted, forgetful of previous conversations, or less emotionally attuned
| Feature | Engaged therapist | Burned-out therapist |
|---|---|---|
| Attunement | Warm, consistent, responsive | Distanced, inconsistent, dismissive |
| Session quality | Personalized, goal-oriented | Formulaic, routine |
| Client progress | Steady growth | Stalled or regressed |
| Alliance strength | Strong, trusting | Fragile, disconnected |
| Communication | Open and responsive | Minimal or delayed |
The therapeutic alliance, the quality of the relationship between client and therapist, is one of the strongest predictors of treatment success. Burnout directly erodes that alliance, often without either party identifying the cause.
What causes burnout in therapy? Underlying factors and stressors
Now that we know what burnout is in therapy, examining why it’s so common is essential for prevention.
Therapist burnout arises from chronic workplace stress, including high caseloads, emotional labor from repeated trauma exposure, insufficient organizational support, and mounting administrative burdens. Measuring these factors is typically done through the Maslach Burnout Inventory (MBI), a validated research tool that assesses all three burnout dimensions. What makes California particularly challenging is the combination of high demand for mental health services, elevated cost of living, and workforce shortages.
Between 35 and 39 percent of US mental health workers reported burnout between 2022 and 2023. California’s numbers are significantly worse. The sheer volume of people seeking care for anxiety, depression, PTSD, and complex trauma places enormous strain on providers, who often absorb that collective weight without adequate recovery time.
Top causes of therapist burnout in California:
- Caseload volume: Many therapists carry 30 or more active clients per week, far exceeding what allows for sustainable emotional engagement.
- Secondary traumatic stress: Regular exposure to trauma narratives gradually erodes a therapist’s own sense of safety and emotional resilience.
- Administrative overload: Billing, documentation, insurance navigation, and compliance paperwork consume hours that could support clinical recovery.
- Inadequate supervision: Early-career therapists especially suffer when they lack mentoring and reflective supervision structures.
- Value misalignment: When clinicians feel their agency’s policies conflict with ethical care, moral distress amplifies burnout risk.
| Stressor | Impact on therapist | Impact on client |
|---|---|---|
| High caseload | Emotional depletion | Less individualized attention |
| Secondary trauma | Detachment and numbness | Felt as coldness or disinterest |
| Administrative burden | Reduced clinical focus | Rushed or cut sessions |
| Poor supervision | Unprocessed emotional buildup | Inconsistent approaches |
| Value conflicts | Disengagement | Fragmented care goals |
Pro Tip: If you’re wondering whether your California therapist or provider organization has burnout safeguards, ask directly how many clients they see per week and whether they receive regular clinical supervision. These are legitimate questions any quality provider should welcome.
For Californians managing ongoing stress alongside these concerns, reviewing coping tips for Californians can also give you more grounding while you navigate the therapy process.
Burnout in therapy: Not just a ‘therapist problem’
With root causes in mind, it’s important to recognize how burnout can ripple out to affect those in therapy directly.
Here’s a reality that rarely gets discussed honestly: when your therapist is burned out, your anxiety treatment, depression recovery, or trauma work doesn’t simply continue as normal at a slightly reduced quality. The evidence shows it can actively stall or reverse your progress. Therapist burnout is linked to poorer therapeutic alliance and worse outcomes across anxiety, trauma, and depression recovery, making burnout-aware providers especially critical in California where prevalence is so high.
For individuals working through trauma, this is especially significant. Trauma recovery requires a deep sense of relational safety. When a therapist’s engagement wanes, even subtly, the nervous system picks up on it. You may feel inexplicably unsafe, dismissed, or ashamed, without understanding why your progress has stopped.
“The quality of care you receive is not just about the techniques a therapist uses. It’s about who is actually present with you in the room.”
Signs that burnout may be affecting your therapy:
- You’ve brought up the same issues multiple times without feeling forward movement
- Your therapist seems to forget important details about your history or goals
- Sessions feel perfunctory, like checkboxes being ticked
- You leave feeling worse than when you arrived, consistently
- Communication between sessions has slowed or become unresponsive
Choosing evidence-based therapy with providers who actively measure outcomes offers one layer of protection. Evidence-based practitioners regularly evaluate whether their methods are working, which creates natural accountability for the quality of care.
Personal growth in therapy requires a therapist who is genuinely invested. Families seeking support for children or teens are particularly vulnerable here, because young people may not have the language to articulate when something in the therapeutic relationship feels off.

Pro Tip: Keep a simple session journal. After each appointment, jot down one sentence about how engaged you felt your therapist was and one about whether you felt heard. Patterns become visible quickly, and this gives you concrete information for conversations with your provider.
Prevention and action: What you can do to protect the therapy process
Understanding the risks is crucial, but what can you do about it as a client or family? Here’s how to safeguard your therapy experience.
Therapist resilience training and mindfulness practices have been shown to reduce burnout effectively, but clients and families also play an active role in shaping the conditions for good care. This isn’t about managing your therapist. It’s about being an informed, empowered participant in your own healing.
Actionable steps to protect your therapy experience:
- Ask about supervision and self-care. When meeting a new provider, ask whether they receive regular clinical supervision. Supervised therapists process difficult cases, which protects both the clinician and you.
- Discuss pacing openly. Especially for trauma recovery, pacing matters enormously. A collaborative approach to session intensity reduces the emotional overload that contributes to both therapist and client exhaustion.
- Request a strengths-focused framework. Prevention through collaborative pacing and focusing on individual strengths has been shown to reduce disengagement on both sides of the therapeutic relationship.
- Watch for red flags early. Don’t wait until you’ve lost six months of progress. If something feels consistently off after three or four sessions, name it.
- Seek agencies with structured support. Group practices with clinical directors, peer consultation, and documented burnout protocols offer more stability than solo practitioners without support networks.
- Use telehealth strategically. For some clients, trauma recovery therapy options via telehealth actually reduce access barriers and make it easier to continue care without logistical stress contributing to dropout.
- Ask about outcome tracking. Providers who use standardized measures to track your progress are less likely to let stagnation go unaddressed.
Pro Tip: If you sense your sessions have stalled, try asking your therapist: “What would progress look like for me over the next few months?” A burned-out provider may struggle to answer with clarity, while an engaged one will have a thoughtful response.
Debates and challenges: Is burnout just an individual problem?
Alongside personal prevention, it’s worth considering how bigger systemic issues shape the therapy landscape in California.
The dominant conversation about therapist burnout still focuses heavily on individual solutions: meditate more, set better limits, practice self-care. But an important counterargument has been gaining traction. Focusing only on self-care may fail to address the structural conditions that cause burnout in the first place. When the building itself is broken, patching the person doesn’t fix the building.
Christina Maslach, one of the foremost researchers on burnout, identifies six organizational areas that matter: workload, control, reward, community, fairness, and values. When one or more of these areas is chronically misaligned, individual coping strategies can only do so much. A therapist meditating after a 30-client week is not solving the problem. They’re managing it.
Questions to ask potential therapy providers:
- How many clients does each therapist carry per week?
- Is clinical supervision built into the schedule, or is it optional?
- How does the practice address therapist wellbeing structurally?
- What happens if a therapist needs to reduce their caseload?
- Does the organization have a documented burnout prevention policy?
| Approach | Focus | Limitation |
|---|---|---|
| Individual self-care only | Person-level coping | Doesn’t address workload or systemic stress |
| Structural reform | Organizational conditions | Slower to implement, requires leadership buy-in |
| Hybrid model | Both person and system | Most effective but least common |
Therapy modalities and outcomes are significantly shaped by the organizational context in which therapy is delivered. The best EMDR or CBT techniques in the world are less effective when the clinician delivering them is stretched far beyond sustainable limits.
Why addressing burnout in therapy means changing the whole system
Here’s an uncomfortable truth that most therapy-focused articles won’t say out loud: as clients and families, you have more power than you realize, and more responsibility than you’re typically given.
The standard advice given to people seeking therapy is essentially passive. Choose wisely, notice red flags, speak up if something feels wrong. That’s all reasonable. But it stops short of acknowledging that real change in the quality of California mental health care requires clients to ask harder questions of the institutions providing that care.
At Revive Health Therapy, we believe what truly supports therapist wellbeing is not a meditation app or a weekend wellness retreat. It’s an organizational commitment to sustainable caseloads, genuine peer support, transparent outcome tracking, and a culture where therapists can say “I am struggling” without career consequences. When providers create those conditions, clients receive measurably better care.
The awkward reality is that burned-out therapists are not bad people. They are often extraordinarily dedicated people working inside systems that were never designed with their wellbeing in mind. And the people who pay the steepest price for that design flaw are the clients those systems are supposed to serve.
Choosing a provider is not just a clinical decision. It’s a vote for a certain kind of practice culture. When you ask questions about supervision, caseloads, and structural support, you’re not being difficult. You’re being a smart consumer of mental health care, and you’re participating in a slow but meaningful shift in what quality therapy looks like in California.
Get support from burnout-aware therapy providers in California
Knowing what to look for in a therapist is the first step. Taking action is the next one.
At Revive Health Therapy, we take provider wellbeing seriously because we know it directly affects your outcomes. Our team uses evidence-based psychotherapy options including EMDR, CBT, and mindfulness-based approaches, delivered by clinicians who receive ongoing supervision and work within sustainable caseloads. Whether you’re exploring reasons to seek psychotherapy for the first time or need specialized trauma recovery evidence-based care, we offer in-person sessions in Walnut Creek and Oakland, as well as telehealth across California. Sliding-scale fees and insurance accepted. You deserve care that’s built to last.
Frequently asked questions
How can I tell if my therapist is experiencing burnout?
Watch for emotional distancing, less personalized feedback, or frequent scheduling disruptions. The three burnout dimensions, emotional exhaustion, depersonalization, and reduced accomplishment, often surface as feeling like your therapist is physically present but mentally elsewhere. A direct, respectful conversation with your provider is always a reasonable first step.
Does therapist burnout affect therapy outcomes for clients?
Yes, significantly. Research links therapist burnout directly to early client dropout and stalled recovery, particularly for those in anxiety or trauma-focused treatment. The effects are not minor and can delay meaningful progress by months.
What can clients do if they suspect burnout is affecting their therapy?
Raise your concern directly with your therapist and discuss adjustments to pacing or approach. Collaborative pacing and a strengths focus have been shown to reduce disengagement on both sides. If the dynamic doesn’t shift, seeking a provider at an agency with built-in burnout prevention practices is a legitimate and healthy choice.
Is burnout the same as depression or a mental disorder?
No. Burnout is classified as an occupational phenomenon under ICD-11, not a diagnosable mental illness like depression. This distinction matters because it means burnout is primarily addressed through workplace and organizational change, not just clinical treatment of the individual experiencing it.
Recommended
- Psychotherapy in California 2026: Evidence & Options – Revive Health Therapy
- Step by step therapy guide for Californians 2026 – ReviveHealthTherapy
- Online Therapy in California | Revive Health Therapy
- Practical mental health coping tips for Californians – Revive Health Therapy
- What a massage therapist does: Care for pain and recovery