
TL;DR:
- Recent FDA updates and clinical research show that hormone therapy effectively improves mood during perimenopause, contradicting outdated fears. Different hormone replacement options have varying impacts on anxiety and depression, with transdermal estradiol and micronized progesterone offering the most mood-friendly profiles. Personalized treatment combining hormone therapy and psychotherapy provides the most comprehensive support for emotional health in adults experiencing hormonal shifts.
Many adults in California quietly assume that hormone medication is either too risky or too narrowly focused on menopause to be relevant to their anxiety or depression. That assumption is increasingly outdated. Recent FDA guidance from 2026 has reshaped how clinicians and patients understand the safety profile of hormone therapy, and a growing body of clinical research confirms what many perimenopausal adults have experienced firsthand: when hormones shift, mood follows. This guide explains what the evidence actually shows, which types of hormone medication matter for emotional health, and how to access care that combines hormonal and psychological support.
Table of Contents
- Understanding hormone medication types and FDA guidance
- Hormone medication’s impact on anxiety and depression symptoms
- Nuances and best practices in hormone medication for emotional health
- Accessing hormone medication and supportive care in California
- Why hormone medication deserves a fresh look in mental health care
- Explore mental health and hormone therapy support in California
- Frequently asked questions
Key Takeaways
| Point | Details |
|---|---|
| Updated FDA guidance | The FDA removed some hormone therapy black box warnings, reflecting lower mood treatment risks when started early after menopause. |
| Types of hormone medication | Four main therapies include systemic combination, estrogen-alone, progestogen-alone added to estrogen, and topical vaginal estrogen. |
| Mood symptom improvement | Hormone medication improves anxiety and depression symptoms in many perimenopausal women, especially combined with antidepressants. |
| Delivery methods matter | Transdermal estradiol is safer and often more effective for mood symptoms than oral formulations. |
| Integrated care approach | Combining hormone medication with psychotherapy and professional monitoring supports the best mental health outcomes. |
Understanding hormone medication types and FDA guidance
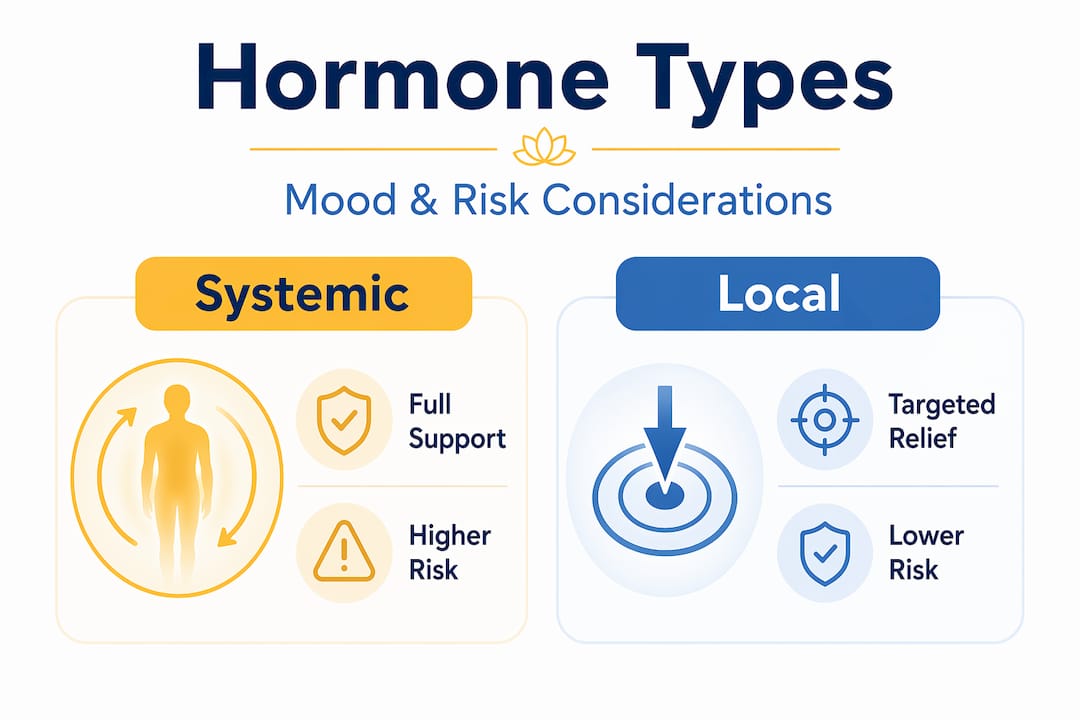
When most people hear “hormone medication,” they picture a single drug. In reality, four primary hormone replacement therapies are recognized by the FDA for menopausal symptoms, and each carries a different risk profile and set of applications.
Here is how they break down:
- Systemic combination therapy (estrogen plus progestogen): Used for adults with a uterus to protect against endometrial cancer. Most commonly prescribed for moderate to severe menopause symptoms affecting sleep, mood, and cognition.
- Estrogen-alone therapy: Prescribed only for adults who have had a hysterectomy. Estrogen without progestogen avoids the mood complications that some progestogens introduce.
- Progestogen-alone added to estrogen: Used when estrogen alone is the primary treatment but uterine protection is needed. The specific progestogen formulation chosen has significant implications for mood outcomes.
- Topical vaginal estrogen: Treats localized symptoms with minimal systemic absorption, making it relevant for those who need hormonal support without broader cardiovascular or breast tissue exposure.
One of the most significant developments in 2026 is that the FDA approved labeling changes removing boxed warnings for cardiovascular disease, breast cancer, and dementia from many hormone therapy products. These warnings had been in place since the early 2000s after a study that was later found to have methodological limitations affecting how broadly its findings applied. The revised guidance helps providers and patients make decisions based on current evidence rather than two-decade-old caution.
| Therapy type | Best for | Mood relevance | Key risk consideration |
|---|---|---|---|
| Systemic combination | Full symptom relief, intact uterus | High, but progestogen choice matters | Depends on progestogen type |
| Estrogen-alone | Post-hysterectomy adults | Strong positive mood effects | Lower risk than combination |
| Progestogen add-on | Uterine protection with estrogen | Variable, formulation dependent | Synthetic progestins can worsen mood |
| Topical vaginal estrogen | Localized symptoms | Minimal systemic mood effect | Very low systemic risk |
Providers choose among these based on symptoms, health history, and your personal priorities. Understanding the role of psychotherapy in mental health alongside hormone therapy is equally important, since emotional symptoms rarely respond to hormones alone.
Hormone medication’s impact on anxiety and depression symptoms
The mood benefits of hormone therapy are more specific and measurable than most people realize. This is not about a vague sense of feeling better. Researchers are now tracking discrete anxiety and depression scores before and after treatment.
A 2026 clinical trial found that estradiol and dydrogesterone combined with the antidepressant escitalopram produced significantly better outcomes on both anxiety and depression scales than either treatment used alone in perimenopausal women. The takeaway is not that hormones replace antidepressants. It is that the combination creates a synergistic effect that neither can achieve independently.
Testosterone tends to get overlooked in this conversation. It is not just relevant to libido. A retrospective study found that testosterone replacement therapy in women improved depression, irritability, and anhedonia (the inability to feel pleasure) by over 50%, with symptom gains actually increasing over time rather than plateauing. For adults experiencing persistent low motivation or emotional numbness alongside perimenopausal changes, this is worth asking a provider about directly.
Key findings worth knowing:
- Mood symptoms improve in 70 to 80% of perimenopausal women within 3 to 6 months of starting hormone treatment.
- Combination hormone and antidepressant therapy consistently outperforms either alone in clinical comparisons.
- Testosterone therapy’s mood effects build gradually, meaning short trial periods may not capture the full benefit.
- Hormonal shifts during perimenopause directly affect serotonin and GABA pathways, which is why mood instability often precedes other physical symptoms.
Pro Tip: If your anxiety or depression worsened in your late 30s or 40s and antidepressants have not fully worked, ask your provider to check FSH and estradiol levels. Perimenopause can begin years before the last period, and hormonal fluctuation may be the missing piece of your treatment picture.
For adults already working with a therapist, evidence-based depression treatments and psychotherapy for anxiety are natural partners to hormone medication rather than alternatives.
Nuances and best practices in hormone medication for emotional health
Getting hormone therapy right for mood is not as simple as starting a prescription. The type of hormone, the delivery method, and the dosing schedule all produce meaningfully different outcomes for anxiety and depression.
Here are the four most important clinical nuances to understand before starting:
-
Avoid sequential progestin schedules if mood is your primary concern. Sequential regimens cycle progestin for 10 to 14 days per month to mimic a menstrual pattern. During those progestin-heavy days, many adults experience anxiety, irritability, and low mood spikes. Micronized progesterone or a continuous low-dose regimen significantly reduces this risk in patients with anxiety history.
-
Request transdermal estradiol, not oral estrogen, when mood is the treatment goal. Oral estrogen is processed through the liver, which affects how it influences brain chemistry and increases clotting risk. Transdermal estradiol patches maintain steady hormone levels throughout the day, producing a more consistent serotonin-supporting effect without the peaks and troughs of oral dosing.
-
Ask about allopregnanolone testing if mood worsens on progestin. Allopregnanolone is a metabolite of progesterone that acts on GABA receptors in the brain, producing calming effects in some people and paradoxical anxiety in others. Testing this level can help identify why some patients feel worse on progestin and guide a switch to body-identical micronized progesterone.
-
Start within 10 years of menopause onset. The “timing hypothesis” in hormone research is well-supported. Women who begin hormone therapy within the first decade after menopause experience better mood outcomes and face lower cardiovascular and cognitive risks than those who start later. Waiting is not neutral.
Pro Tip: Print out your hormone therapy questions before your appointment. Providers in busy practices often default to the most commonly prescribed option. Asking specifically about “transdermal estradiol” and “micronized progesterone” signals that you understand the importance of evidence-based therapy choices and want a personalized plan.
Accessing hormone medication and supportive care in California
California is one of the better states for accessing hormone therapy combined with mental health support, but the system still requires some navigation. Here is what to prioritize:
- Find a provider with dual fluency in hormones and mental health. Gynecologists are familiar with estrogen but may not think in terms of depression scores. Psychiatrists understand mood disorders but may not order hormonal panels. Look for integrative providers or women’s health specialists who connect both areas.
- Confirm perimenopause with objective testing. FSH (follicle-stimulating hormone) levels, estradiol, and progesterone testing give your provider a baseline. Symptoms alone are often insufficient for precise dosing decisions.
- Know your delivery options before the appointment. Pills, patches, creams, vaginal rings, and suppositories all exist. Each has a different absorption rate, convenience level, and side effect profile. Patches and gels tend to work best for mood.
- Build in psychotherapy from the start. Hormone medication addresses the biological substrate of mood. It does not replace the cognitive and emotional work that therapy provides. The two work together in ways neither can replicate alone.
- Monitor consistently. Blood levels after 6 to 8 weeks help calibrate dosing. Keep a mood journal to track emotional shifts between appointments. This data matters when adjusting treatment.
- Use seeking psychotherapy in California resources early. Waiting until symptoms are severe limits your options. Early treatment typically means lower doses, faster response, and better long-term outcomes.
According to FDA-aligned individualized assessment guidance, hormone therapy benefits depend on age, symptom severity, and health history. There is no single right answer, which is why personalized consultation matters more than any general protocol.
Why hormone medication deserves a fresh look in mental health care
Here is something most mental health content will not say directly: the fear of hormone therapy has caused real harm. For roughly 20 years, millions of perimenopausal and menopausal adults were steered away from hormone medication based on a study that was misapplied to a much broader population than the one it actually examined. The result was unnecessary suffering, poorly managed depression, and an overdependence on antidepressants that did not address the hormonal root cause.
Modern hormone therapies initiated early after menopause carry substantially lower risks than previously understood, and their mood benefits are now well-documented across multiple trial designs. This is not a minor update. It represents a significant shift in what responsible mental health care looks like for perimenopausal adults.
What we find most important at Revive Health Therapy is this: the details of hormone therapy selection matter enormously, and most people do not know what questions to ask. The wrong progestogen can worsen anxiety. The wrong delivery method can undermine mood stability. A provider who defaults to a standard prescription without considering your specific mood profile may be leaving the most effective treatment on the table. Advocating for yourself in that appointment is not optional; it is part of the treatment.
Hormone medication can also reduce reliance on antidepressants in carefully selected patients. That is not to say antidepressants should be abandoned. But for someone who has been on SSRIs for years with incomplete relief and is now in perimenopause, the conversation about adding hormone therapy has a real evidence base behind it. Combining evidence-based therapy with informed hormone treatment is what individualized care actually looks like.
Explore mental health and hormone therapy support in California
Navigating anxiety, depression, and hormonal changes at the same time is genuinely hard. The good news is that you do not have to treat them as separate problems. At Revive Health Therapy, we work with adults across California who are looking for mental health support that meets them where they are, whether that means seeking psychotherapy in California in person at our Walnut Creek or Oakland locations, or connecting through secure telehealth.
Our therapists use CBT, EMDR, and mindfulness-based approaches to address the emotional and psychological dimensions of mood disorders that hormone medication alone cannot reach. If you are weighing your telehealth therapy options or trying to figure out how to choose the right therapy type for your situation, we can help you think it through. We accept insurance and offer sliding-scale fees to keep care accessible at every income level.
Frequently asked questions
What types of hormone medication are available for anxiety and depression in perimenopausal adults?
The FDA recognizes four types of menopausal hormone replacement therapy: systemic combination therapy, estrogen-alone therapy, progestogen-alone therapy added to estrogen, and topical vaginal estrogen, each of which can support mood symptoms depending on the individual’s profile.
Are hormone medications safe for long-term use regarding heart disease and cancer risks?
FDA-approved label changes in 2026 removed boxed warnings for cardiovascular disease, breast cancer, and probable dementia from menopausal hormone therapies, reflecting evidence that risks are substantially lower when treatment begins within 10 years of menopause onset.
Can hormone medication replace antidepressants for anxiety and depression?
Hormone medication is usually part of a broader treatment plan rather than a standalone replacement; research shows that estradiol combined with escitalopram outperforms either treatment alone, suggesting the most effective approach is often combination therapy.
How can I safely access hormone medication for mood disorders in California?
Work with a provider experienced in both hormonal and mental health care, complete hormonal lab testing to confirm perimenopause, and pursue individualized assessment that factors in your age, health history, and symptom severity before starting any prescription.
Does the method of hormone delivery affect its effectiveness for mood symptoms?
Yes. Transdermal estradiol patches are preferred for mood and anxiety because they deliver steady hormone levels throughout the day and do not carry the increased clotting risk associated with oral estrogen.
Recommended
- Mental health self-care ideas for anxiety and depression – Revive Health Therapy
- Why Use Psychotherapy for Anxiety: Real Solutions – ReviveHealthTherapy
- Manage anxiety with proven therapies in California 2026 – Revive Health Therapy
- 7 Types of Therapy for Anxiety and How They Can Help You – ReviveHealthTherapy